Transformation of lymphoma
Slow-growing (low-grade) lymphoma can sometimes change (transform) into a faster-growing (high-grade) type of lymphoma. High-grade lymphomas need different treatment.
On this page
Why does transformation happen?
Who might be affected by transformation?
When might transformation happen?
What is transformation?
Transformation is when a slow-growing (low-grade) lymphoma changes into a faster-growing (high-grade) lymphoma. It is important to know if your lymphoma has transformed because it will require different treatment.
Most low-grade lymphomas do not transform.
If a low-grade lymphoma does transform, it is most likely to develop into a type of high-grade lymphoma called diffuse large B-cell lymphoma (DLBCL). Occasionally, it can transform to other types, such as Burkitt lymphoma, other high-grade B-cell lymphomas or Hodgkin lymphoma.
Very occasionally, people who have a high-grade lymphoma relapse in the future with a low-grade lymphoma. Doctors aren’t certain why this happens. They think it might be because tiny, undetectable levels of low-grade lymphoma were present at diagnosis, which later caused a relapse. The high-grade lymphoma might have been caused by transformation of low-grade lymphoma at a very early stage.
Why does transformation happen?
Low-grade lymphomas are mostly made up of small, slow-growing cells. These might be mixed in with a few faster-growing cells, or some of the slow-growing cells might mutate (change genetically) over time to become fast-growing. If the number of faster-growing lymphoma cells increases, the lymphoma can begin to behave more like a high-grade lymphoma.
Who might be affected by transformation?
In most cases lymphoma does not transform.
Transformation can happen in any type of low-grade lymphoma but it is most common in follicular lymphoma. Every year, transformation affects around 2 to 3 in every 100 people with follicular lymphoma. Over the course of 10 years, it will transform in up to a third of people with follicular lymphoma.
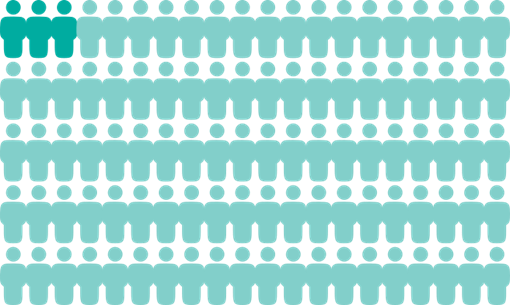
2 to 3 people in every 100 with follicular lymphoma experience transformation each year.
Other types of low-grade lymphoma transform less frequently. Types of lymphoma that sometimes transform include:
- chronic lymphocytic leukaemia or small lymphocytic lymphoma (CLL/SLL) (this transformation is called Richter syndrome)
- marginal zone lymphomas (including gastric MALT lymphoma, non-gastric MALT lymphoma, nodal marginal zone lymphoma and splenic marginal zone lymphoma)
- Waldenström’s macroglobulinaemia and other lymphoplasmacytic lymphomas
- a slow-growing type of Hodgkin lymphoma called nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL).
Scientists are trying to identify changes in lymphoma cells that can help them work out who is most at risk of transformation. Currently, there is no reliable way of predicting whether lymphoma is likely to transform in an individual.
Nothing you do (or have done) can make transformation more or less likely to happen.
Can treatment affect the risk of transformation?
There is no clear evidence that any of the treatments for low-grade lymphomas (for example, chemotherapy or antibody therapy) increase or decrease the risk of the lymphoma transforming.
Some studies have suggested that early treatment of lymphoma could reduce the risk of transformation. Other studies have found that early treatment has no effect on the risk of transformation. At present, doctors think there is no difference in the risk of transformation between people who have an initial period of active monitoring (watch and wait) for low-grade lymphoma and people who have treatment straightaway.
When might transformation happen?
Transformation is possible at any time after diagnosis. Occasionally, low-grade lymphoma has already transformed when it is diagnosed. In this case, your tests might show that you have a mixture of high-grade and low-grade lymphoma.
In a few people, lymphoma might transform within months of diagnosis. In others, lymphoma might transform many years later. Some research suggests that the risk of lymphoma transforming becomes lower around 15 to 20 years after diagnosis.
Your medical team check for signs of transformation at all your appointments.
Symptoms of transformed lymphoma
If your lymphoma transforms, it might affect the same part of your body as before, or a different part. The symptoms you experience depend on where the lymphoma is growing. The symptoms may be the same or different to those you’ve experienced previously. The most common signs and symptoms of transformed lymphoma include:
- swollen lymph nodes that are growing quickly
- rapid swelling of your liver or your spleen (an organ of your immune system)
- weight loss, night sweats or fevers (B symptoms)
- high levels of certain chemicals found on blood tests.
If you don’t have symptoms, your lymphoma is very unlikely to have transformed.
If you think your lymphoma might have transformed, contact your medical team straightaway. You don’t have to wait for your next appointment.
The symptoms of transformed lymphoma can be similar to signs that your lymphoma has come back (relapsed). Relapsed lymphoma and transformed lymphoma need different treatment so it is important for your medical team to know which you have. If they think your lymphoma might have transformed, they are likely to perform a PET/CT scan and a biopsy to confirm it.
Outlook
Transformed lymphoma can be difficult to treat but treatment options are improving all the time. Many people can be successfully treated.
Your individual outlook varies greatly depending on your individual circumstances. Your medical team are best placed to advise you on your outlook. They can use the results of your tests and other individual factors (for example, your age and general health, the exact type of lymphoma you have and what treatment you’ve already had) to help them judge how likely you are to respond to a particular treatment.
If you choose to research survival statistics, be cautious. Survival statistics don’t tell you what your individual outlook is – they only tell you how a group of people with a similar diagnosis did over a period of time. They are usually measured at least 5 or 10 years after treatment. This means that statistics only tell you how people did in the past. Those people might not have received the same treatment as you. The outlook for transformed lymphoma is much better now than it was before antibody therapies and other targeted therapies were available to treat lymphoma.
Back to top
Treatment
There is no standard treatment for transformed lymphoma. Your medical team recommends the most appropriate treatment for you based on:
- the type and stage of the transformed lymphoma
- the treatment you’ve already had and how you responded to it
- your age and general health
- the results of your tests and scans
- your preferences.
If you haven’t had it before, you are likely to be offered the standard treatment option for the type of high-grade lymphoma your lymphoma has transformed into. For most types of transformed lymphoma, this is likely to be chemotherapy combined with antibody therapy (‘chemo-immunotherapy’ – for example, R-CHOP or Pola-R-CHP).
If you’ve already had the standard chemotherapy or chemo-immunotherapy regimen for your type of lymphoma, you might be offered a stronger chemotherapy regimen. If your lymphoma responds to this and your general health is good enough, your medical team might suggest an autologous (self) stem cell transplant. Stem cell transplants involve intensive chemotherapy and are not suitable for everyone.
If you need more than one course of treatment for transformed lymphoma, you might be offered CAR-T cell therapy, a bi-specific antibody, or an allogeneic (donor) stem cell transplant.
Your medical team might ask if you would like to take part in a clinical trial. Find out more about clinical trials, and search for a trial that might be suitable for you, on Lymphoma TrialsLink.
I was called in by the haematology team following a CT scan and expected them to say it was a single low-grade swelling. However, this time it was a transformation to high-grade and treatment would start as soon as chemotherapy could be arranged. I was shocked as only one enlarged node could be felt. My mind was in a spin and I was a little upset but the team were great with the explanations and care.
Research
Scientists are testing many different treatments in clinical trials for lymphoma. Although many of these trials are not open to people with transformed lymphoma, a few are.
Clinical trials are being conducted to test new treatment options as well as those currently available, looking at using them in different situations and in new treatment combinations. Current research is focussed on:
- Antibody therapies that bind to two different targets (one on lymphoma cells and one on T cells, which helps the T cells find and destroy the lymphoma cells). These are called ‘bispecific’ antibodies.
- Antibody–drug conjugates (antibodies joined to chemotherapy drugs). The antibody sticks to a protein on the surface of lymphoma cells and carries the chemotherapy drug directly to it.
- CAR T-cell therapy, which involves modifying your own immune cells to recognise and destroy lymphoma cells.
- Cell signal blockers, which block signals that B cells send to help them divide or stay alive.
- Immunomodulators, which change how your immune system works.
- Programmed cell death inducers, which block proteins that keep lymphoma cells alive.
- Checkpoint inhibitors, which stop lymphoma cells hiding from your immune system.
Some of these might be available to you through a clinical trial. Speak to your doctor if you are interested in taking part in a clinical trial. To find out more about clinical trials or to search for a trial that might be suitable for you, visit Lymphoma TrialsLink.
Back to top