CNS prophylaxis
This information is about treatment to prevent lymphoma spreading to your central nervous system (CNS). Most people have a low risk of their lymphoma spreading to the CNS and do not need CNS prophylaxis.
We have separate information on lymphoma that starts in the CNS.
On this page
What is CNS prophylaxis?
Who might need CNS prophylaxis?
Having CNS prophylaxis
What is CNS prophylaxis?
Rarely, some types of lymphoma can spread to your central nervous system (CNS). The CNS is the part of your body that controls all your body’s functions. It includes your brain, your spinal cord and your eyes.
Lymphoma that has spread to the CNS can be difficult to treat. If you are at high risk of your lymphoma spreading to your CNS, your medical team might offer you treatment that aims to stop it developing. This is called ‘CNS prophylaxis’. Prophylaxis is a medical word for treatment designed to prevent something.
Most people have a low risk of their lymphoma spreading to the CNS and do not need CNS prophylaxis. Your medical team will only suggest CNS prophylaxis if you have certain types of lymphoma, or risk factors that make your type of lymphoma more likely to spread to the CNS. However, the main priority is always to treat the lymphoma you have, rather than to prevent a lymphoma that might develop. If your medical team think that CNS prophylaxis would interfere with your treatment, they are unlikely to recommend it even if you have risk factors. This might be the case for older people or people with kidney or heart problems, who are less likely to tolerate CNS prophylaxis in addition to their recommended lymphoma treatment.
We have separate information on lymphoma that starts in the CNS, or is already affecting your CNS when it is diagnosed.
Who might need CNS prophylaxis?
People with low-grade non-Hodgkin lymphoma or Hodgkin lymphoma are unlikely to need CNS prophylaxis.
CNS prophylaxis is part of the standard treatment for very fast-growing types of non-Hodgkin lymphoma, such as Burkitt lymphoma or lymphoblastic lymphoma.
For other types of high-grade non-Hodgkin lymphoma, your medical team consider your individual risk factors.
Diffuse large B-cell lymphoma (DLBCL) can occasionally spread to the CNS. This only happens in around 5 out of every 100 cases. Most people with DLBCL do not develop lymphoma in their CNS and do not need CNS prophylaxis. However, there are some factors that might increase your risk of lymphoma spreading to your CNS. If you have DLBCL, your medical team is likely to recommend CNS prophylaxis if you have any of these factors:
- lymphoma in three or more places outside your lymph nodes
- lymphoma in any of the following places:
- testicles
- kidneys
- adrenal glands (glands on top of your kidneys that make hormones to help control your blood pressure, your body’s response to stress and how fast the cells in your body work)
- blood vessels (intravascular lymphoma)
- four or more of the following:
- high levels of a chemical called lactate dehydrogenase (LDH) in your blood
- aged over 60
- lymphoma that is stopping you working or being active
- lymphoma in two or more places outside your lymph nodes
- stage 3 or 4 lymphoma
- lymphoma in your kidneys or your adrenal glands (note that this also warrants CNS prophylaxis without other factors).
Your medical team might also suggest CNS prophylaxis if you have DLBCL affecting your breasts or womb (uterus).
Many doctors use the same criteria as DLBCL to decide whether or not to offer CNS prophylaxis to people with other types of high-grade non-Hodgkin lymphoma, including:
- primary mediastinal large B-cell lymphoma
- follicular lymphoma that has changed (transformed) into a faster-growing type.
They might also consider using these criteria for people with T-cell lymphomas.
Speak to your medical team if you are worried about your risk of developing lymphoma in your CNS. They can advise you on whether or not you need CNS prophylaxis. They can also explain the risks and benefits of this type of treatment.
Having CNS prophylaxis
Your CNS is protected from harmful chemicals and infections by a layer of cells and blood vessels called the ‘blood–brain barrier’. This separates your brain from your bloodstream and only lets certain substances through. Your blood–brain barrier is important to protect your brain, but it can make it difficult for drugs to get into your CNS.
Some drugs can cross the blood–brain barrier but others can’t. Some drugs need to be given in high doses for enough to cross the blood–brain barrier and reach the CNS.
Depending on the drug your medical team recommends, and the dose that needs to reach your CNS, you might have CNS prophylaxis in one or both of the following ways:
- Through a drip into a vein (an intravenous infusion). This is the most common way to have it.
- As an injection into the fluid surrounding your brain and spinal cord (an intrathecal injection). This method is used less often in current practice.
Intravenous CNS prophylaxis
Intravenous CNS prophylaxis involves having chemotherapy through a drip into a vein. It can be used for drugs that cross the blood–brain barrier. Most people who need CNS prophylaxis have it this way.

Having chemotherapy through a drip
The most common drug given intravenously for CNS prophylaxis is called methotrexate. It has to be given in high doses for enough of it to reach the CNS. This is known as high-dose methotrexate, or HD-MTX. It can affect how well your kidneys work, so it might not be suitable for you if you already have reduced kidney function. In this case, you might be offered intrathecal CNS prophylaxis instead.
You typically have two or three doses of high-dose methotrexate for CNS prophylaxis. Each dose takes around 2 to 4 hours. You might have these doses 2 to 3 weeks apart after you’ve finished all your chemotherapy. You have blood tests in between doses to check your blood counts and to make sure your liver and kidneys are working well enough to keep having treatment.
The most common side effects of high-dose methotrexate include a low white blood cell count (neutropenia), low levels of platelets (thrombocytopenia), a sore mouth, feeling or being sick, and changes in the way your kidneys and liver work. These side effects usually go away once you finish treatment.
Your medical team should tell you about any side effects you might develop depending on the drugs you are having and your individual circumstances.
Intrathecal chemotherapy
Intrathecal CNS prophylaxis involves having chemotherapy injected directly into the fluid surrounding your brain and spinal cord (the cerebrospinal fluid, or CSF). This is usually done through a lumbar puncture.
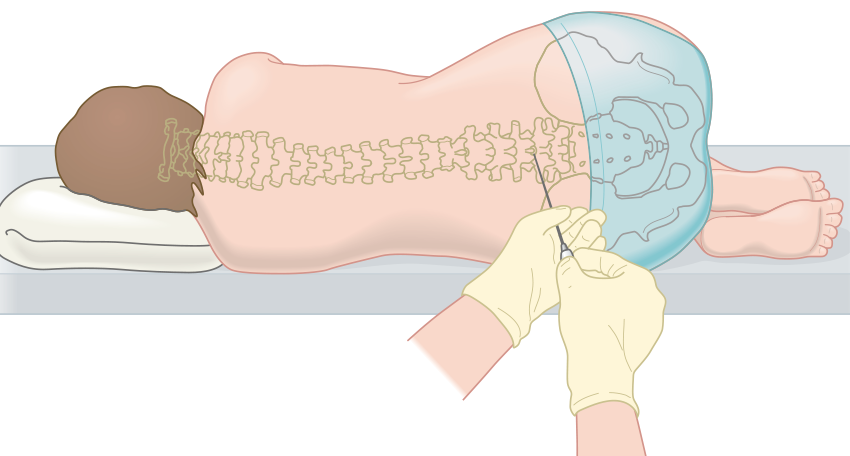
Having a lumbar puncture
Intrathecal treatment avoids the blood–brain barrier so the chemotherapy can reach your CNS in higher doses than when it’s given intravenously. It doesn’t reach the rest of your body. However, chemotherapy given this way only enters some parts of your CNS and can’t get into your brain tissue.
Only certain drugs can safely be given intrathecally. The most common drug given this way is methotrexate. For CNS prophylaxis, you usually have intrathecal methotrexate once during each cycle of standard chemotherapy. The whole process usually takes around 20 minutes.
However, scientific evidence supporting intrathecal methotrexate is mixed and there are potential side effects. Many consultants therefore no longer offer it.
You might be offered intrathecal methotrexate if you need CNS prophylaxis and your kidneys are not working as well as they should. This could make intravenous CNS prophylaxis unsafe for you because it could reduce your kidney function further. Intrathecal methotrexate doesn’t affect your kidneys.
Occasionally, you might have intrathecal CNS prophylaxis as well as intravenous CNS prophylaxis. This is most likely to be the case if you have DLBCL affecting your testicles.
The most common side effects of intrathecal methotrexate include a headache or dizziness, a high temperature, stiffness in your back, neck or shoulders, shivering or trembling, and feeling or being sick. Your medical team should tell you about any side effects you might develop depending on the drugs you are having and your individual circumstances.